Splenic lymphoma, particularly Splenic Marginal Zone Lymphoma (SMZL), is a rare and indolent (slow-growing) form of non-Hodgkin lymphoma (NHL). It primarily affects B-cells and occurs in the spleen but can extend to other organs, such as the bone marrow, blood, and lymph nodes. Despite its slow progression, SMZL can become aggressive over time, presenting unique challenges for diagnosis and treatment.
What is Splenic Lymphoma?
Splenic lymphoma is a type of non-Hodgkin lymphoma (NHL) that originates in the marginal zone of the spleen. The marginal zone is a specialized area of the spleen that helps in immune response regulation.
While SMZL typically manifests as an indolent disease, it can sometimes transform into a more aggressive form of lymphoma, known as Diffuse Large B-Cell Lymphoma (DLBCL), requiring more intensive treatment.
Symptoms and Diagnosis
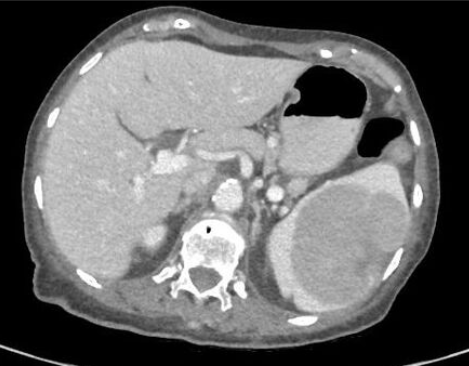
The hallmark symptom of SMZL is splenomegaly (enlargement of the spleen), which can lead to discomfort or pain in the left side of the abdomen. Other symptoms may include fatigue, weight loss, and signs of anemia or thrombocytopenia (low platelet count). SMZL is also associated with autoimmune disorders like autoimmune hemolytic anemia (AIHA), in which the immune system attacks its own red blood cells.
Because it presents slowly and may remain asymptomatic for long periods, the disease is often diagnosed incidentally during imaging tests for unrelated issues or when symptoms such as spleen enlargement become apparent.
A definitive diagnosis is made using a combination of clinical evaluation, imaging (such as CT scans), blood tests, and biopsy. Histopathological examination of spleen tissue reveals the characteristic infiltration of marginal zone B-cells.
Treatment Options for Splenic Lymphoma
Treatment for SMZL depends on the stage of the disease and whether it is causing symptoms. Many patients with indolent SMZL may not require immediate treatment but instead undergo “watchful waiting,” where their condition is closely monitored for any progression. When symptoms appear or the disease progresses, several treatment options are available:
Chemotherapy and Immunotherapy
Chemotherapy is often combined with immunotherapy for more aggressive disease. The most common treatment regimen involves rituximab, a monoclonal antibody that targets the CD20 protein on B-cells. Rituximab is often used in combination with chemotherapy agents like cyclophosphamide or bendamustine.
Targeted Therapy
Targeted therapies have shown promise in treating SMZL, especially when the disease relapses. Drugs such as ibrutinib (Imbruvica) and zanubrutinib (Brukinsa) target Bruton’s tyrosine kinase (BTK), an enzyme critical for B-cell survival and function. Other promising therapies include lenalidomide (Revlimid), which has been approved for use in relapsed or refractory marginal zone lymphoma.
Splenectomy
In cases where the spleen is severely enlarged or causing discomfort, a splenectomy (removal of the spleen) may be recommended. This procedure helps alleviate symptoms, such as pain and low blood counts, and is often used in conjunction with other therapies.
Radiation Therapy
Radiation therapy can be used in cases where the lymphoma is localized to the spleen or other organs. It is particularly useful in relieving symptoms caused by an enlarged spleen.
Antiviral Treatment for Hepatitis C
In some patients, SMZL is associated with chronic hepatitis C virus (HCV) infection. Treating HCV with antiviral medications can sometimes result in a reduction of lymphoma symptoms, and in some cases, it may even cure the lymphoma.
Prognosis and Survival Rates
The prognosis for patients with SMZL varies widely depending on several factors, including the extent of disease progression and response to treatment. On average, survival rates for patients with SMZL can be quite favorable, with a 10-year survival rate ranging from 67% to 95%, depending on the stage at diagnosis and the presence of complications.
However, approximately one-third of patients experience rapid disease progression or transformation into an aggressive lymphoma, which significantly affects the prognosis and may require more intensive treatments.
Advances in Research and Treatment
Recent advancements in the understanding of the molecular and genetic underpinnings of SMZL are leading to more personalized treatment approaches. Researchers are studying the epigenetic modifications and the tumor microenvironment of SMZL to uncover novel therapeutic targets.
The development of new drugs, including targeted therapies and immunotherapies, holds promise for improving outcomes, especially for patients with relapsed or refractory disease.
Clinical trials are ongoing to explore the efficacy of newer agents like acalbrutinib (Calquence) and mosunetuzumab (Lunsumio) in treating SMZL, which could expand the treatment options available for this rare lymphoma.
Immunotherapy and CAR-T Cell Therapy in Splenic Lymphoma
Immunotherapy has become an essential component of treatment for many forms of lymphoma, and research into its application for splenic lymphoma is ongoing. A novel form of immunotherapy, CAR-T (chimeric antigen receptor T-cell) therapy, has shown promise in treating aggressive forms of lymphoma, including those that may evolve from SMZL.
In CAR-T therapy, a patient’s own T-cells are genetically modified to recognize and attack lymphoma cells. While this treatment is still in its early stages for SMZL, ongoing trials are exploring its effectiveness in treating both refractory and relapsed cases. Early data suggests that this could provide a new avenue for patients whose disease is resistant to conventional treatments like chemotherapy or targeted therapy.
The Role of the Microbiome in Splenic Lymphoma
Emerging research has also highlighted the potential influence of the microbiome—the community of bacteria and other microorganisms in the body—on the development and progression of lymphoma, including splenic lymphoma.
Studies have shown that certain bacterial infections, particularly those linked to autoimmune diseases or chronic inflammation, might trigger or worsen the condition. For example, there is a well-documented association between hepatitis C and SMZL.
Research into the microbiome’s role suggests that balancing microbial communities could help modulate immune responses and potentially reduce the risk of lymphoma progression. This area of study is still evolving, but it may one day lead to probiotic or antibiotic-based therapies as adjunct treatments for patients with SMZL.
In Closing
Splenic lymphoma, particularly SMZL, is a slow-growing but potentially serious form of lymphoma. While many patients experience indolent disease with favorable long-term survival, a subset of patients faces rapid disease progression that requires more aggressive interventions.
Advances in targeted therapy and personalized treatment approaches are improving outcomes for those affected by this rare disease. Continued research into the genetic and molecular factors of SMZL promises to further refine treatment strategies and offer hope for more effective management of this condition.
For the latest treatment options, patients are encouraged to consult with their healthcare provider to explore available therapies, including those through clinical trials.
FAQs on Splenic Lymphoma
Q: What is splenic lymphoma?
A1: Splenic lymphoma, also known as splenic marginal zone lymphoma (SMZL), is a rare form of non-Hodgkin lymphoma (NHL) that originates in B-cells, a type of white blood cell. This lymphoma typically affects the spleen but can also involve the bone marrow, blood, and lymph nodes.
Q: What are the symptoms of splenic lymphoma?
A: Symptoms of splenic lymphoma can vary. In the early stages, many individuals may have no symptoms, and the disease might be discovered during routine exams or blood tests. When symptoms do appear, they may include:
Abdominal discomfort due to spleen enlargement (splenomegaly)
Fatigue
Breathlessness
Easy bruising or bleeding
Infections due to low blood cell counts
Abnormal protein buildup in the blood, which can lead to headaches, confusion, nosebleeds, and blurred vision.
Q: What causes splenic lymphoma?
A: The exact cause of splenic lymphoma is unclear. However, long-term infection with hepatitis C (HCV) has been linked to the development of SMZL. It’s important to note that not everyone with HCV will develop lymphoma.
Q: How is splenic lymphoma diagnosed?
A: SMZL is usually diagnosed through a combination of physical exams, imaging tests (like CT scans or ultrasounds), blood tests, and biopsies of affected tissues. Doctors may also perform a bone marrow biopsy if the disease affects the bone marrow.
To read more, click here.